October 24, 2024
Two new studies show many don’t understand management of severe allergic reactions
BOSTON (Oct. 24, 2024) – Anaphylaxis can come on suddenly and without warning, and because its symptoms can be fatal, it is scary for those who encounter it. Two new studies being presented at this year’s American College of Allergy, Asthma and Immunology (ACAAI) Annual Scientific Meeting in Boston show it is not only patients and caregivers who misunderstand how best to treat anaphylaxis: emergency medical professionals often follow incorrect protocols for treating severe allergic reactions.
“We know early recognition of anaphylaxis and treatment with epinephrine improves outcomes,” says Sasha Alvarado, DO, Co-Director of Quality and Safety for the Division of Immunology, Allergy and Retrovirology at Baylor College of Medicine. Joni Chow, DO, Pediatric Resident at Baylor College of Medicine, San Antonio and lead author of the study explained, “We surveyed 96 patients and caregivers in an allergy clinic waiting room to evaluate knowledge of anaphylaxis and desired components of an anaphylaxis action plan. The results demonstrate the need for better education of allergy patients to recognize and treat anaphylaxis appropriately.”
Although 95% of the respondents in the study were prescribed epinephrine and 73% said they were comfortable with recognizing anaphylaxis symptoms, only 14% of respondents said they were very likely to use epinephrine first for anaphylaxis. The following were barriers to using epinephrine:
- Not sure which symptoms to treat (40.6%)
- Hesitant to go to the emergency room (24%)
- Hesitant to call 911 (17.7%)
- Not sure how to use epinephrine auto-injectors (11.5%)
- Feared needles (5.2%)
A second study examined the differences across emergency medical services (EMS) in the United States regarding protocols used in the prehospital treatment of anaphylaxis. The study performed an analysis of statewide anaphylaxis protocols to identify gaps in the recognition of anaphylaxis and to provide areas for improvement in prehospital management.
“Many EMS anaphylaxis protocols are incomplete and/or outdated,” says Carly Gunderson, DO, lead author of the study. “The discrepancies include variations in the definition of anaphylaxis as well as in treatment.”
30 states – those with a mandatory Advanced Cardiac Life Support (ACLS) protocol were included in the study. Of the 30 states, only 50% (15) included gastrointestinal symptoms in the definition of anaphylaxis, and only 40% (12) included neurologic manifestations. 47% (14) used a two-organ system definition. For anaphylactic reactions, 100% (30) of protocols recommended diphenhydramine and epinephrine. 90% (27) recommended albuterol if respiratory symptoms were present, 73% (22) recommended intravenous fluids, and 60% (18) recommended steroids. Epinephrine was the first line recommendation for anaphylaxis in 97% (29) of protocols. 25 states (83%) allowed epinephrine autoinjectors and 17 (57%) provided autoinjectors.
The authors said it was surprising that many EMS protocols did not consider gastrointestinal or neurologic manifestations to be a component of anaphylaxis. Additional outdated recommendations included the use of steroids and first-generation antihistamines. Many protocols did not permit or provide epinephrine autoinjectors, despite their convenience and effectiveness.
Abstract Title: UNDERSTANDING OF ANAPHYLAXIS MANAGEMENT AMONG ALLERGY PATIENTS AND COMPONENTS OF A PATIENT-CENTERED ANAPHYLAXIS ACTION PLAN (See full abstract below)
Presenter: Joni Chow, DO
Abstract Title: DISCREPANCIES IN ANAPHYLAXIS PROTOCOLS ACROSS EMERGENCY MEDICAL SERVICES IN THE UNITED STATES – OPPORTUNITIES FOR IMPROVEMENT (See full abstract below)
Presenter: Carly Gunderson, DO
For more information about anaphylaxis, or to find an allergist in your area, visit AllergyandAsthmaRelief.org. The ACAAI Annual Scientific Meeting is Oct. 24-28. For more news and research from the ACAAI Scientific Meeting, go to our newsroom and follow the conversation on X/Twitter #ACAAI24.
About ACAAI
The American College of Allergy, Asthma & Immunology (ACAAI) is a professional medical organization of more than 6,000 allergists-immunologists and allied health professionals, headquartered in Arlington Heights, Ill. Founded in 1942, the College fosters a culture of collaboration and congeniality in which its members work together and with others toward the common goals of patient care, education, advocacy, and research. ACAAI allergists are board-certified physicians trained to diagnose allergies and asthma, administer immunotherapy, and provide patients with the best treatment outcomes. For more information and to find relief, visit AllergyandAsthmaRelief.org. Join us on Facebook, Pinterest, Instagram and X/Twitter.
A001
DISCREPANCIES IN ANAPHYLAXIS PROTOCOLS ACROSS EMERGENCY MEDICAL SERVICES IN THE UNITED STATES – OPPORTUNITIES FOR IMPROVEMENT
C. Gunderson*1, S. Lopez2, K. Lukose3, N. Akar-Ghibril2, 1. Pembroke Pines, FL; 2. Hollywood, FL; 3. Boca Raton, FL.
Introduction: Across the United States, there are significant inconsistencies in the protocols used by Emergency Medical Services (EMS) in the prehospital treatment of anaphylaxis. These discrepancies include variations in the definition of anaphylaxis as well as treatment recommendations. This study performed an analysis of statewide anaphylaxis protocols to identify gaps in the recognition of anaphylaxis and to provide areas for improvement in prehospital management.
Methods: States with mandatory or model state-wide ACLS protocols were included (total of 30). Each allergic reaction and/or anaphylaxis protocol was reviewed – emphasis was placed on the definitions used to identify reactions and treatment algorithms.
Results: Of the 30 states, only 50% (15) included gastrointestinal symptoms in the definition of anaphylaxis, and only 40% (12) included neurologic manifestations. 47% (14) used a two-organ system definition. For anaphylactic reactions, 100% (30) of protocols recommended diphenhydramine and epinephrine. 90% (27) recommended albuterol if respiratory symptoms were present, 73% (22) recommended intravenous fluids, and 60% (18) recommended steroids. Epinephrine was the first line recommendation for anaphylaxis in 97% (29) of protocols. 25 states (83%) allowed epinephrine autoinjectors and 17 (57%) provided autoinjectors.
Conclusion: Many EMS anaphylaxis protocols are incomplete and/or outdated. Surprisingly, many protocols do not consider gastrointestinal or neurologic manifestations. Additionally, many contain outdated recommendations, including the use of steroids and first-generation antihistamines. Despite the convenience of epinephrine autoinjectors, many protocols do not permit or provide them. Given the frequency of EMS activation for allergic reactions, our communities would benefit from standardized protocols using current evidence-based guidelines for the management of anaphylaxis.
A002
UNDERSTANDING OF ANAPHYLAXIS MANAGEMENT AMONG ALLERGY PATIENTS AND COMPONENTS OF A PATIENT-CENTERED ANAPHYLAXIS ACTION PLAN
J. Chow*1, M. Stahl1, S. Alvarado2, 1. San Antonio, TX; 2. Houston, TX.
Introduction: Anaphylaxis is life-threatening, and early recognition improves outcomes. We aimed to assess patients’ and caregivers’ understanding of recognition and management of anaphylaxis and identify preferred components of a patient-centered action plan.
Methods: We developed a survey instrument assessing knowledge of anaphylaxis and desired components of an anaphylaxis action plan. Surveys were completed by 96 patients/caregivers in an allergy clinic waiting room.
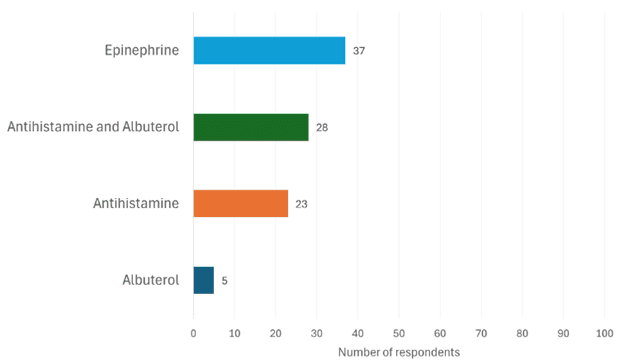
Results: 95.8% of respondents were prescribed epinephrine. 73% agreed or strongly agreed with feeling comfortable with recognizing anaphylaxis symptoms, though only 14% correctly identified symptoms requiring epinephrine. Although 85% stated that antihistamines do not prevent the need for epinephrine, 23.7% would still treat with antihistamine first during an anaphylactic episode. In the setting of rash and wheezing after suspected allergen exposure, 64.5% would inject epinephrine while 10.8% would drive to the emergency room first. The following were barriers to using epinephrine: not sure which symptoms to treat (40.6%), not sure how to use epinephrine auto-injectors (11.5%), feared needles (5.2%), hesitant to call 911 (17.7%), hesitant to go to the emergency room (24%). 36.5% had an anaphylaxis action plan (AAP). The top desired components rated very or somewhat important on an AAP included: section for management of mild (non-anaphylactic) allergic reaction symptoms (93%), visuals of how to inject epinephrine (87.6%), visuals of anaphylaxis symptoms (81%).
Conclusion: This study demonstrates the need for better education of allergy patients to recognize and treat anaphylaxis appropriately and supports the use of visuals in creating a patient-centered AAP.
Which medication would you use first if you or your child developed rash and wheezing after a suspected allergen exposure?